- July 15, 2026
- Posted by: Josh Knoll
- Category: Pain Management Billing

We all know that pain management billing doesn’t behave like general physician billing. It’s a lot more complex. This is because the patient here can generate charges for imaging guidance, drug administration, facility fees, and monthly care management – all on a single visit. And if you get one modifier wrong, a $400 radiofrequency ablation claim comes back, denied.
Where Pain Management Stands Today
Today, most adults struggle with chronic pain that frequently limits their daily life or work where the age is the biggest driver. In a report by CDC, it is seen that chronic pain affects just 12.3% of adults aged 18–29, but climbs to 36.0% in adults 65 and older, meaning more than one in three seniors is living with persistent pain.
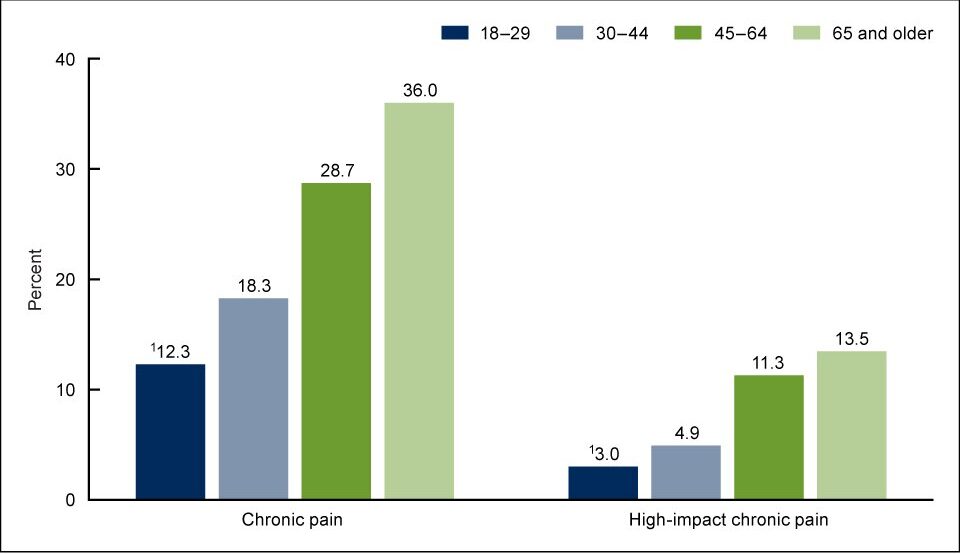
That’s not a demographic footnote; it’s the entire reason Medicare volume dominates the pain management payer mix, and why practices that don’t understand Medicare’s coverage rules for pain management billing struggle from day one.
Why the Specialty Keeps Growing
- Aging population: Musculoskeletal degeneration doesn’t slow down. Also, it is seen that osteoarthritis alone affects roughly 32.5 million U.S. adults and the majority of people over 55 are already showing radiographic spinal degeneration.
- The opioid pullback: After the big change of the CDC’s 2022 opioid prescribing guideline pushed the non-opioid and non-pharmacologic therapy to first-line status, interventional procedures like injections, ablations and stimulators have become a growth engine rather than a niche add-on.
- Medicare’s reimbursement: CMS didn’t have a code that captured the actual work of managing a chronic pain patient month over month until the code G3002/G3003 was created in 2023
- ASC migration: Procedures that used to require a hospital outpatient department can now be performed in an ASC at a fraction of the facility cost, reshaping how practices structure their billing entirely.
With better imaging and more precise diagnostics, today, more patients receive a defensible diagnosis and a documented reason for intervention. It is no longer a vague chronic back pain note that can’t support medical necessity, which is another big reason, along with the rest, as to why the demand is rising.
Understanding Different Types of Pain and Their Impact on Medical Billing
Every claim starts with an accurate clinical picture, and this is why understanding what type of pain drives the ICD-10 code and medical necessity; all becomes important
- Acute pain: short-duration, tied to a specific injury or event. Usually straightforward from a billing standpoint because the diagnosis code is tied directly to the inciting event.
- Chronic pain: persisting beyond three months, per CMS’s own definition used for the CPM program. This is where the documentation burden increases sharply.
- Neuropathic pain: nerve-origin pain, be it for diabetic neuropathy or post-herpetic neuralgia requires diagnostic specificity. This is because payers scrutinize these codes closely, as neuropathic pain codes support high-reimbursement procedures like spinal cord stimulation.
- Cancer pain: often billed under palliative or oncology-adjacent codes, with different medical necessity thresholds than non-malignant chronic pain.
- Musculoskeletal pain: the highest-volume category where patients are struggling with arthritis, disc disease, facet syndrome and the primary driver of injection and ablation volume.
- Post-operative pain: time-limited by definition; payers expect this to resolve and will flag prolonged billing under this diagnosis.
- Complex Regional Pain Syndrome (CRPS): a diagnosis payers hold to a high evidentiary standard, since it often justifies costlier interventions like sympathetic blocks or stimulator trials.
- Other chronic conditions: fibromyalgia, chronic pelvic pain, and headache/migraine syndromes, each having its own LCD nuances depending on MAC jurisdiction and its own billing nuance.
Some Common Procedures and Treatments
| Procedure | What It Treats | Billing Note |
|---|---|---|
| Medication Management | Ongoing pharmacologic care | Often billed alongside E/M or CPM codes. |
| Epidural Steroid Injection | Radiculopathy and disc-related pain | Imaging guidance is bundled and is not separately billable. |
| Facet Joint Injection | Facet-mediated axial pain | Requires level-specific CPT coding (64490–64495). |
| Radiofrequency Ablation (RFA) | Facet-mediated pain requiring longer-lasting relief | Documentation must include two positive diagnostic medial branch blocks before billing. |
| Cervical RFA | Cervical facet joint pain | Uses a separate CPT code set from lumbar and sacral RFA procedures. |
| SI Joint Injection | Sacroiliac joint dysfunction | Medicare coverage varies significantly by Medicare Administrative Contractor (MAC). |
The Multidisciplinary Reality of Pain Management:
Today, payers increasingly expect to see more than one lever being pulled. A comprehensive pain care plan typically touches exhaustive assessment documentation, medication management with a clear rationale for each agent, interventional procedures tied to a specific diagnosis and psychological or behavioral health input, especially before device implants. Along with rehabilitation and functional goals, not just pain score. In fact, billing for pain management requires more attention because of it’s:
- High per-procedure cost and every claim gets more payer scrutiny than a routine office visit here.
- Multiple payers, multiple rulebooks have the same CPT code can have entirely different coverage criteria under Medicare, a commercial LCD-equivalent policy, and workers’ comp.
- Prior authorization is the norm, not the exception, especially for stimulators, pumps, and repeat RFAs.
- Imaging guidance is baked into the code, not billed separately and a mistake that shows up constantly in audits.
- Documentation has to prove failed conservative treatment before payers will cover injections or ablation.
- Medical necessity is procedure-specific. A diagnosis that supports an epidural doesn’t automatically support an RFA.
- Modifier complexity is constantly increasing. 50 for bilateral, 59 for distinct procedural service, 25 for a separately billable E/M on a procedure day, where each one has to be backed by chart documentation, not just appended out of habit.
- Drug billing (buy-and-bill) adds inventory and reimbursement-timing risk on top of the procedural coding itself.
This matters for billing because payers explicitly want to know if the practice tries a multidisciplinary approach, especially before approving costlier procedures.
Other reasons why pain management billing and medicine deserve more attention than they usually get include:
- Benefits verification needs to confirm frequency limits and prior visit history for the specific procedure being scheduled, not just active coverage.
- Prior authorization should be initiated the moment a procedure is scheduled, not the day before; its turnaround times of 5–10 business days are common even for routine injections.
- Charge capture is where fluoroscopy time, drug units, and modifier-eligible bilateral work most often get missed, because it happens in the gap between the procedure room and the billing system.
Where Pain Management Practices Actually Lose Money
Today, mistake in pain management billing never shows up as a denial. It shows up as revenue that was simply never billed, or billed and quietly written off and mostly because of:
- Missed authorizations: a procedure gets performed before the authorization clears, and the claim is dead on arrival.
- Modifier errors: bilateral procedures billed without modifier 50, or a same-day E/M billed without modifier 25 support.
- Missed fluoroscopy or drug billing: units administered but never captured in the charge ticket.
- Wrong units on drug codes: a common and entirely preventable underpayment source.
- Repeat injections: When some treatment is billed outside frequency windows without documentation justifying medical necessity for the exception.
- Documentation gaps: the clinical note doesn’t support the level of service actually billed.
- Delayed follow-up on denials: timely filing windows close while a denial sits in a queue.
- Underpayments that go unchallenged: payers routinely reimburse below contracted rates, and most practices don’t have a systematic process to catch it.
Documentation Checklist that every few Pain management provider need to track:
| Procedure | Required Documentation |
|---|---|
| Epidural | MRI or imaging findings, failed conservative treatment, documented pain score, and specific diagnosis. |
| RFA | Two positive diagnostic medial branch blocks with documented pain relief response. |
| Spinal Cord Stimulator | Psychological evaluation and documented trial period results. |
| Facet Injection | Imaging findings and documented history of conservative therapy. |
The Codes behind Pain Management Billing
It is no secret that the pain billing draws on several code sets simultaneously and a claim usually needs all of them working together starting from:
- ICD-10-CM: the diagnosis, increasingly required at a specific level (laterality, chronicity, associated psychosocial factors)
- CPT: the procedure or service performed
- HCPCS Level II: drugs, supplies, and CMS-specific codes like G3002/G3003
- Modifiers: bilateral, distinct procedure, repeat procedure, and E/M-on-procedure-day flags
- POS codes: office vs. ASC vs. hospital outpatient, which changes both the fee schedule and which party bills the facility component
- Diagnosis-to-procedure linkage: many LCDs list the exact ICD-10 codes that will support medical necessity for a given CPT code, and anything outside that list gets denied automatically.
Key CPT Codes to Know in Pain Management:
Pain management coding is undoubtedly far more complex. This is because pain management coders need to understand that CPT 62323, which is used for lumbar/sacral epidural steroid injections with imaging guidance and fluoroscopy, should not be billed separately. Also, in certain pain treatment dealing with bilateral procedures typically requires Modifier 50. Additionally, code 64635 is reported for lumbar or sacral radiofrequency ablation (RFA) and requires proper documentation of positive diagnostic medial branch blocks before billing. Not to forget, 99490 is used for Chronic Care Management (CCM) and should not be confused with chronic pain management codes, as it cannot be billed in the same month as G3002 or G3003 for the same patient. And this is mainly because G3002 covers the first 30 minutes of monthly chronic pain management services, including pain assessment, care planning, medication management, and care coordination, while G3003 is an add-on code for each additional 15 minutes of medically necessary services. So, for a mid-sized practice, any coding errors here aren’t rounding errors.
Why the Site of Service Matters in Pain Management Billing:
This decision shapes practice economics more than almost any other billing choice. Not to forget that ASC billing usually means faster patient throughput and lower cost per case, but it requires two clean claims instead of one, along with a breakdown in coordination between facility and physician billing, which is at times a common source of denials and doesn’t exist in an office-based model.
| Factor | ASC | Office-Based |
|---|---|---|
| Facility Fee | Billed separately by the ASC | Not applicable — practice absorbs overhead |
| Professional Fee | Physician bills separately from the facility | Physician bills the full global fee |
| Reimbursement | 30–45% lower facility cost than hospital outpatient, per 2024 CMS reimbursement parity rules covering 14 additional interventional procedures | Generally higher per-procedure reimbursement with no facility fee split |
| Coding | Requires separate facility and professional claims | Single claim covers both components |
| Documentation | Facility and physician documentation must independently support the same procedure | One documentation set, but it must support the entire global fee |
Pain management billing is undoubtedly a highly detailed specialty that requires close attention, as even a minor mistake can result in denied claims, delayed payments, or revenue loss. From managing buy-and-bill reimbursements to understanding the differences between Medicare and commercial insurance policies, billing teams must navigate several complex requirements, or else countless denials may cause losses for the pain management center or clinic.
The Biggest Billing Challenges in Pain Management
- Prior authorization volume and turnaround time
- Procedure and frequency limitations that shift by payer
- Documentation burden that keeps growing with each ICD 10 update
- Controlled substance and drug billing restrictions
- Constant coding updates (new G-codes, revised RVUs, shifting LCDs)
- Underpayments that go unchallenged
- Missing or expired prior authorization
- Medical necessity is not clearly supported in the note
- Frequency limits exceeded without exception documentation
- Modifier errors (50, 59, 25 applied incorrectly or omitted)
- Diagnosis-to-procedure mismatch against the payer’s coverage policy
- LCD violations where a code was billed outside the region’s approved diagnosis list
- Duplicate claims from timing or resubmission errors
- Provider credentialing issues, especially for newer associates
- Appeals processes that consume staff time disproportionate to the claim value
- Staffing shortages in specialty trained coders, which are arguably the root cause of most of the above
Pain Management Billing Demands Specialized Expertise
With all these complications and confusion, keeping track of everything can be overwhelming at times. Moreover, with some payer policies changing quarterly, sometimes without meaningful notice often creates chaos too. Additionally, documentation requirements keep expanding faster than templates get updated. While the volume of appeals keeps growing, most practices don’t even have dedicated appeals staff handling pain management billing services.
This is why specialized RCM partners like SunKnowledge tend to add the most measurable value. Be it payer-specific denial tracking or underpayment recovery, we offer the solution that most in-house teams often struggle with.
How Outsourcing Improves Pain Management Billing
Today, the case for outsourcing isn’t generic; it’s specific to what this specialty demands:
- Specialized coders who know the difference between 64490 and 64493 without looking it up mid claim
- Payer knowledge that comes from working hundreds of pain claims across multiple MACs and commercial plans, not just one practice’s payer mix
- Reduced denials by catching modifier and frequency errors before submission, not after
- Faster reimbursement through cleaner first-pass claims and quicker appeal turnaround
- Scalable staffing that doesn’t collapse when one coder goes on leave
And SunKnowledge excels in all these because we ensure a tailored, customized solution to all your billing problems and not a generic RCM applied to pain management as an afterthought. With dedicated coders who track LCD differences by MAC jurisdiction, a denial management process built around the specific reasons pain claims get rejected, and prior authorization support structured around the procedures, we do it all at a cost effective rate. For practices trying to close the gap between what they’re billing and what they’re actually collecting, let our expertise help you recover what is left on the table.